“Sensing Breast” Reconstruction (MS-TRAM)

Doctor Helena Puonti has been able to create the “Sensing Breast” reconstruction technique by adding a microneurovascular approach to the traditional Free Muscle Sparing TRAM* method.
Innovative Breast Reconstructive Surgery
Since 2001, Helena Puonti has been developing a ground-breaking breast reconstruction method that allows the restoration of a high degree of sensation to the breasts after free MS-TRAM reconstruction. Doctor Helena Puonti’s dissertation was published in 2017 and the research included results on ca. 100 patients.
The shape of the newly reconstructed breast is important for the patient’s quality of life. But Helena Puonti realised that even more important is the fact that the breast also feels. This is how the idea of the Sensing Breast method was born.
The Sensing Breast method is a further developed version of MS-TRAM breast reconstruction method. The MS-TRAM* flap is the best transplant for breast reconstruction after mastectomy. It is soft and can naturally acquire the necessary shape. It is possible to reconstruct a round and, if necessary, large breast from it.
* MS-TRAM stands for Muscle-Sparing Transverse Rectus Abdominis Myocutaneous flap and microneurovascular describes the method of the flap connection.
Sensing Breast Improving Day-to-Day Life
As with other things in life, not always do we remember to appreciate the importance of something until we lose it. And the same goes for the sensitivity of your breasts.
There are many examples, of how not having sensation on the breasts can affect one’s everyday life. Without sensation, a woman can not feel a hot coffee, tea, or soup spilled on her or feel the pain if the sun is burning and damaging the skin of the breast. Imagine holding a baby in your arms or hugging your kids, without being able to feel their loving embrace.

In 2017, just days before the publication of Doctor Puonti’s study, NY Times wrote an article on the subject showcasing the problems women all around the world face after the traditional breast reconstruction and highlighting the need for the Sensing Breast method.
We are here to help You.
If you would like to hear more about Your breast reconstruction options and if you would be eligible for the Sensing Breast reconstruction, you can access Helena Puonti’s consultation quickly and without a referral.
Why choose Clinic Helena:
- World-class expertise in breast reconstruction, using the most modern methods.
- Helena Puonti’s unique Sensing Breast-method – available only at Clinic Helena.
- Online consultation available.
- We help you with all travel arrangements including visas and invitations.
Sensing Breast – Method Explained
In the Sensing Breast technique, the skin and fatty tissue from the lower abdominal area are transplanted to the site of the removed breast. Both the blood vessels and the nerves are grafted and connected to the blood vessels and nerves in the chest. The traditional method only connects the blood vessels.
Donor site in the abdomen is then closed directly. The abdominal muscles remain almost intact. A patient of Doctor Puonti’s has even delivered a baby after this procedure.
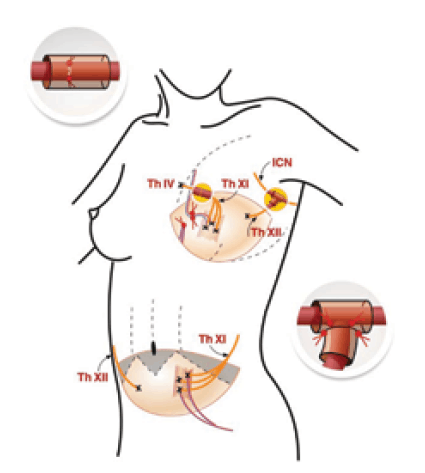
In the figure, the blood vessels are marked in red and blue and nerves in yellow.
Epigastric inferior blood vessels are connected to intramammaric vessels.
Intercostal nerves Th XI and XII have been connected to intercostal Th IV and intercostobrachial (ICN) nerve.
Nerve coaptation is covered with the NeuraGen-tube, which prevents the nerves from sprouting.
Return of Sensation
The sensation in the reconstructed breast returns gradually.
The first signs of sensation appear within about seven months after the nerves are sutured, and then skin sensation – sensitivity to cold, heat, and pain – gradually starts returning for up to 2-3 years.

What is important is that joining the nerves did not cause pain syndromes to the patients in the study. On the contrary, after the use of this reconstructive micro-neurovascular technique, there was less pain in the new TRAM breast compared to traditional methods of surgery without suturing the nerve endings.
Helena Puonti’s research is globally-renowned, state-of-the-art study which forms the basis for the PhD thesis she finished in 2017.
Results of the Study
The research has shown that even one nerve of the MS-TRAM flap sutured to a healthy nerve of the breast area can bring good skin sensation to a new breast.
There are cases of complete recovery in which the breast gains normal sensation.
With 2 nerve coaptations of the flap, the sensation recovery improved even further.
After the nerves are connected, the sensation is restored to the TRAM breast to a much greater extent than without the neural coaptation.
According to her research, all breasts regained sensation.
On average, the sensation recovery in the whole group was over half (60%) of the normal breast sensation.
However, there are cases of complete recovery in which the breast gains normal sensation.
Unfortunately, radiotherapy and surgical scarring may impair sensation in the mastectomy area.
Prices
Breast cancer and breast reconstruction prices vary as all surgeries are designed to fulfill the patient’s needs. You can read more about how the prices are determined here.
Sensing Breast Reconstruction Dissertation, Helena Puonti
Effects of microsurgical nerve repair on sensory function after breast reconstruction
Helsinki University, medical science, Finland, 27.01.2017
A beautiful, naturally-shaped, and symmetrical breast mound will be created for a breast cancer patient after mastectomy using a free abdominal flap. The disadvantage with the breast reconstructed with this method is its lack of sensation, even some spontaneous reinnervation takes place from the surrounding tissues.
The objective of the present study was to find and develop a method of dissecting and reconnecting nerves of the abdominal flap and the chest area in order to reconstruct a breast with sensation for the breast cancer patient. The first aim was to find out, which nerves in the chest and the flap, when coapted, would provide the best sensation to the reconstructed breast. The second aim was to investigate whether the dissecting of the nerves causes additional complications in the abdominal flap donor site. The third aim was to develop a better neurorrhaphy technique, using two nerve pedicles. The fourth aim was to assess and qualify the methods of sensory assessment employed in the study.
Focus Group
Breast reconstruction with a free muscle-sparing transverse rectus abdominis myocutaneous flap (ms-TRAM flap) was performed in this study for 96 breast cancer patients in Savonlinna Central Hospital between 2001 and 2013. The reinnervation of the flap was performed in 44 patients with the novel dual neurorrhaphy technique and in 32 with single neurorrhaphy, and 20 breast reconstruction patients without flap reinnervation functioned as a control group.
Sensory Testing
The contralateral healthy breasts of 38 breast reconstruction patients were used as the reference site, and 20 healthy volunteer women participated sensory testing of healthy abdominal skin. The skin sensation of the reconstructed breast was assessed two years after the surgery. In addition, between 2006 and 2013, sensory testing of the skin of the mastectomized breast was performed prospectively before the reconstruction surgery, and the healthy breast, abdominal skin and the reconstructed breast skin were also tested one year after the surgery. Sensory tests included clinical sensory examinations, quantitative sensory tests (QST), skin samples, and neurophysiological somatosensory evoked potentials (SEP). Additionally, a patient questionnaire of patients’ subjective sensory changes was carried out.

Nerve Connection
Both neurorrhaphy techniques provided the reconstructed breast with better skin sensation than without neurorrhaphy, and dual neurorrhaphy resulted in better sensory recovery than innervation with single neurorrhaphy. All available tactile nerves in the chest area proved to be capable of restoring sensation to the ms-TRAM flap breast. No significant complications occurred in the abdominal wall in the flap donor site with either of the neurorrhaphy techniques. Nerve coaptations did not cause pain symptoms, and the increase in the operative time was insignificant.
Sensory Fibre Recovery
The function of large myelinated sensory fibres (i.e. vibration and tactile detection) recovered best. The poorest recovery took place in small unmyelinated sensory fibres (i.e. thermal detection and sharp-blunt discrimination). As a result of breast cancer treatment, tactile and thermal sensitivity of the mastectomized skin was reduced already before breast reconstruction surgery.
Sensory Assessment Methods
All methods of sensory assessment employed in the study could detect the nerve damage caused by the surgery and measure nerve regeneration, with the exception of epithelial nerve fibre density (ENFD) testing, which could not identify nerve regeneration in the comparison of innervated and non-innervated breast reconstructions. Additionally objective SEP proved to be quite an insensitive method in diagnosing nerve damage, they might be suitable for follow-up of its recovery. QST and the clinical sharp-blunt discrimination test were the most sensitive tests both for the identification of sensory damage and nerve regeneration.
Conclusions
Based on this study, we recommend dual neurorrhaphy of the ms-TRAM flap in breast reconstruction for use in clinical practice.



